
FACTSHEET
Considering a feeding tube (PEG)
On this page
- Key points
- When eating and drinking becomes harder
- Reasons to think about a feeding tube
- Why timing matters
- Deciding not to have a feeding tube
- Things to be aware of
- Types of feeding tubes
- Living with a feeding tube
- Choosing to stop using a feeding tube
- Support and questions to help you decide
- Find out more
.png)
Key points
- A feeding tube helps deliver food (nutrition), fluids, and medicine to your body.
- A feeding tube can help you get nutrition with less effort if swallowing is hard. This can help keep your strength and energy.
- Feeding tubes are put in place in an operation called a gastrostomy. Australia has two types of gastrostomy:
- a PEG is put in place using a camera to guide the tube
- a RIG is put in place using an X-ray to guide the tube.
- Studies show that having a feeding tube fitted early can make the gastrostomy operation safer and help maintain your weight.
- You can still eat food and drink fluids if you decide to have a feeding tube.
- After the operation, you’ll learn how to care for the feeding tube, what to put in it, what not to put in it, and how to look after your tube.
- Your healthcare team and decision tools can help you decide if a feeding tube is right for you.
When eating and drinking becomes harder
As MND progresses, the muscles that help you chew and swallow can become weaker. This can make eating and drinking hard. You might:
- take a long time to finish meals
- lose weight
- feel tired
- feel thirsty
- cough or choke when you eat or drink
- find it harder to swallow medicines.
Reasons to think about a feeding tube
If you are finding meals hard or tiring a feeding tube can:
- give essential nutrition to support your body and overall health
- help you maintain or gain weight
- help your body get enough water
- make it easier to take medicine
- help support regular bowel movements
- lower the chance of food and drink going into the lungs when swallowing
- make mealtimes less stressful
- save you time preparing and eating meals.
People can still enjoy food and drink by mouth after they have a feeding tube. Your speech pathologist or dietitian can advise which foods and fluids are easier to manage.
Why timing matters
It can be hard to think about getting a feeding tube.
Having the tube fitted early, when breathing and swallowing are not badly affected, can:
- make the operation safer
- help your body heal faster
- mean you spend less time in hospital
- help to minimise weight loss.
A feeding tube does not stop MND from progressing. However, studies* show that a feeding tube can help people get the right amount of food and drink to slow weight loss.
Research suggests that inserting a feeding tube before a lot of weight is lost (5-10% of normal weight) is most helpful. Keeping weight stable can support overall health and may help some people live longer.
Deciding not to have a feeding tube
If you decide a feeding tube is not for you, your healthcare team will discuss options that feel right for you. For example, how to make swallowing as comfortable as possible.
Things to be aware of
All operations where medicine is used to help you relax or sleep (sedation or anesthetic) may lead to challenges afterwards. With a gastrostomy, these can include:
- pain while you are healing
- germs (infection) around the tube site which can be treated with medicine (antibiotics)
- bleeding or feeling tender around the tube site.
If you have breathing problems, think about having the operation in a hospital that knows about MND care. They will be able to give you special breathing support if needed.
You’ll need to adjust your daily routine to have skin and tube care. The tube may also change how your body looks, which can take time to get used to.
Types of feeding tubes
A feeding tube is inserted via an operation called gastrostomy. A tube is put directly into your stomach through a small cut in your belly. The tube allows liquid food, fluids and medicines to go straight into your stomach. A dietitian will work with you to provide liquid nutrition that is best for you.
It is common for health care workers to use the word PEG when talking about gastrostomy and feeding tubes.
In Australia, there are two main ways to place a feeding tube:
Percutaneous Endoscopic Gastrostomy (PEG)
- PEG takes 30–60 minutes using sedation to make you sleep.
- A thin flexible camera tube (endoscope) is gently passed through your mouth into your stomach so the doctor can see where to place the feeding tube.
- A small cut is made in your belly, and the tube is guided into place.
Radiologically Inserted Gastrostomy (RIG)
- RIG takes 30–60 minutes using a local anesthetic to numb the skin on the belly.
- A soft tube is put directly into the stomach through a small cut in the belly.
- X-rays are used to help guide where the tube is placed.
- This operation is generally for people with breathing problems.
Your doctor will discuss which way is safest and best for you.
Most feeding tubes need to be changed every 12 months. This is usually a simple procedure, so you do not need to stay in hospital.
Living with a feeding tube
After you have a feeding tube, your healthcare team will teach you, or your carer, how to:
- keep the area clean and dry
- rotate and flush the tube safely
- manage feeds and medicines at home and when you’re out.
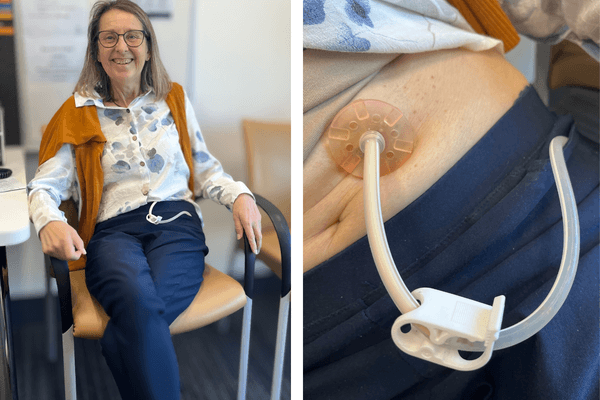
When the feeding tube is not in use, the outer part of the tube can be tucked under your clothes. It can be secured with medical-grade tape or a specially designed pouch to hold the tube close to your body and out of sight during daily activities.
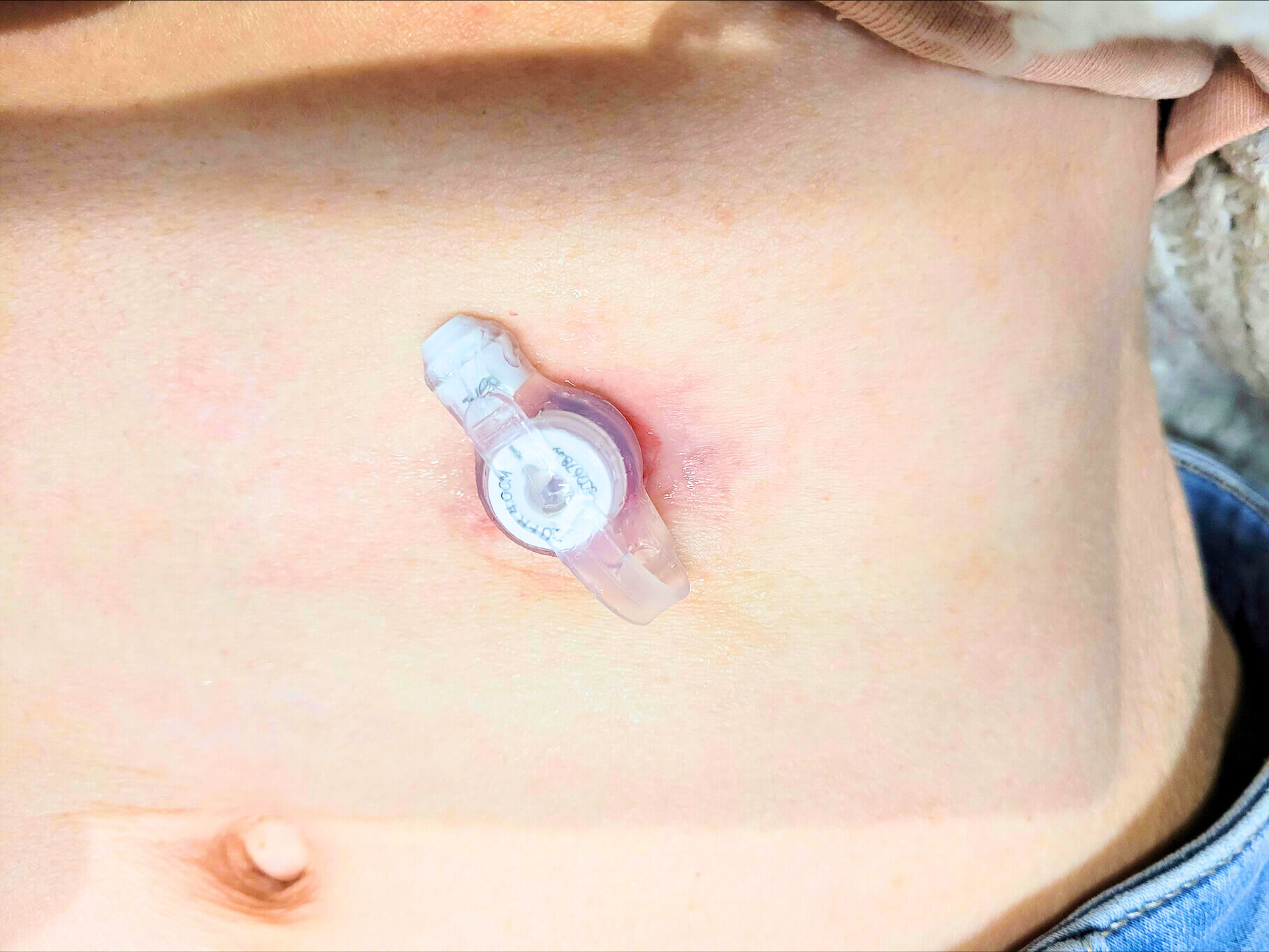
Once the opening on your stomach has healed, you may be able to change to a low-profile tube (button).
A button sits flat against your skin and is only connected to the feeding tube during feeds. This can be more comfortable and less bulky under your clothes.
Choosing to stop using a feeding tube
Your thoughts about using a feeding tube may shift as your MND progresses. You can choose to stop your tube feeds and flushes at any time, if that is your preference.
It is a good idea to talk about your preferences with your family and healthcare team before you get the feeding tube. You can also write your wishes in your advance care plan.
Talk often with your healthcare team about your wishes.
Support and questions to help you decide
You don’t have to decide alone. To help you decide, you can talk with your:
- family
- medical specialist (eg. neurologist or palliative care doctor)
- dietitian and/or speech pathologist
- general practitioner (GP).
You might also like to try the online PEG Ed Decision Tool and the MND Decision Tool: gastrostomy and MND. These tools can help you explore your choices and think about what matters most to you.
Questions you may want to ask your MND or specialist team if you are thinking about having a feeding tube:
- What are the reasons to have the operation now rather than wait?
- What if I decide not to have a feeding tube?
- Are there any potential problems given my current breathing and food needs?
- Will I still be able to eat and drink if I want?
- Which type of gastrostomy operation is safest for me?
- How long will I be in hospital and what will healing be like?
- How does having a feeding tube affect my mouth care?
- Will it be hard for my family and carers to help manage the tube?
- How will I bath, shower or swim?
- How does a tube feeding feel?
- Will having a feeding tube affect my bowel movements?
- What happens if I change my mind after I’ve had a feeding tube put in?
- What will the feeds and equipment cost me?
Find out more
- PEG Ed: The Flinders Medical Centre has a dedicated website, known as PEG Ed, designed to educate people around gastrostomy feeding and includes a decision making tool. The site includes various videos by people living with MND who have considered gastrostomy.
- myTube: developed by SITraN – the Sheffield Institute for Translational Neuroscience, it is an educational resource relevant to everyday life, made in collaboration with people living with MND.
- MND Decision Tool: gastrostomy and MND: This tool is part of a suite of support tools designed to help people with MND discuss their preferences with their family and MND health professionals, developed by Dr Anne Hogden.
- For more personalised advice, talk to your GP, neurologist, clinical team or your local MND Association.
Acknowledgements
- Elizabeth Kapur, Natarsha Emerson and Amy Brown from Flinders Medical Centre, and Simone Reid from MND Queensland for their clinical review and guidance.
- Members of the MND Lived Experience Network (LEN) whose insights ensure this resource reflects the needs and experiences of people living with MND.
- Lynnley Selig for generously sharing her photos to support this resource.
Sources
Bond, L.; Ganguly, P.; Khamankar, N.; Mallet, N.; Bowen, G.; Green, B.; Mitchell, C.S. A Comprehensive Examination of Percutaneous Endoscopic Gastrostomy and Its Association with Amyotrophic Lateral Sclerosis Patient Outcomes. Brain Sci. 2019, 9, 223. https://doi.org/10.3390/brainsci9090223
Wei Q, Ou R, Chen Y, Chen X, Cao B, Hou Y, Zhang L, Shang H. RNM-01 Weight stability is associated with longer survival in amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener. 2019 Nov;20(sup1):309-326. doi: 10.1080/21678421.2019.1647001. PMID: 31702466
Li, JY., Sun, XH., Cai, ZY. et al. Correlation of weight and body composition with disease progression rate in patients with amyotrophic lateral sclerosis. Sci Rep 12, 13292 (2022). https://doi.org/10.1038/s41598-022-16229-9
Dourado Junior MET, Dourado LC, Santana GC, Vale SHL, Leite-Lais L. Impact of weight loss and disease progression on survival in ALS: insights from a multidisciplinary care center. Arq Neuropsiquiatr. 2025 Oct;83(10):1-9. doi: 10.1055/s-0045-1812029. Epub 2025 Oct 15. PMID: 41092967; PMCID: PMC12527597
White S, Zarotti N, Beever D, Bradburn M, Norman P, Coates E, Stavroulakis T, White D, McGeachan A, Williams I, Hackney G, Halliday V, McDermott C; HighCALS group. The nutritional management of people living with amyotrophic lateral sclerosis: A national survey of dietitians. J Hum Nutr Diet. 2021 Dec;34(6):1064-1071. doi: 10.1111/jhn.12900. Epub 2021 Apr 24. PMID: 33786908
Son B, Lee J, Ryu S, Park Y, Kim SH. Timing and impact of percutaneous endoscopic gastrostomy insertion in patients with amyotrophic lateral sclerosis: a comprehensive analysis. Sci Rep. 2024 Mar 26;14(1):7103. doi: 10.1038/s41598-024-56752-5. PMID: 38531942; PMCID: PMC10965990
Sulistyo A, Abrahao A, Freitas ME, Ritsma B, Zinman L. Enteral tube feeding for amyotrophic lateral sclerosis/motor neuron disease. Cochrane Database Syst Rev. 2023 Aug 10;8(8):CD004030. doi: 10.1002/14651858.CD004030.pub4. PMID: 37579081; PMCID: PMC10413437
Tran K, Hayes HA, Bromberg M. A prospective observational study of decision-making by patients with amyotrophic lateral sclerosis upon recommendation for PEG enteral feeding tubes. Nutr Clin Pract. 2025 Jun;40(3):623-629. doi: 10.1002/ncp.11290. Epub 2025 Mar 18. PMID: 40102061; PMCID: PMC12049567.
Gastrostomy Feeding in Motor Neurone Disease, Flinders Medical Centre