
How research and the medical system develop medicines for MND in Australia
Published: June 2023
According to research, the medicine Riluzole can prolong life with motor neurone disease (MND).1 Riluzole is the only medicine for treatment of the disease available in Australia.2
By contrast, people living with MND in the United States of America (USA) can access three medicines: Riluzole, Edaravone and Relyvrio and just this month, Qalsody (previously Tofersen) which can all slow the progress of MND.3,4,5 But currently Australians cannot access Qalsody, Edaravone and Relyvrio through our medical system.
Why don’t people living with MND in Australia have access to medicines like Edaravone? And how can scientists develop medicines sooner?
We looked at what helps a medicine progress from scientific experiments to doctors being able to prescribe it for MND in Australia. With better access to medicines, more people with MND can have greater choice over living with such a terrible disease.
How do we find a new medicine?
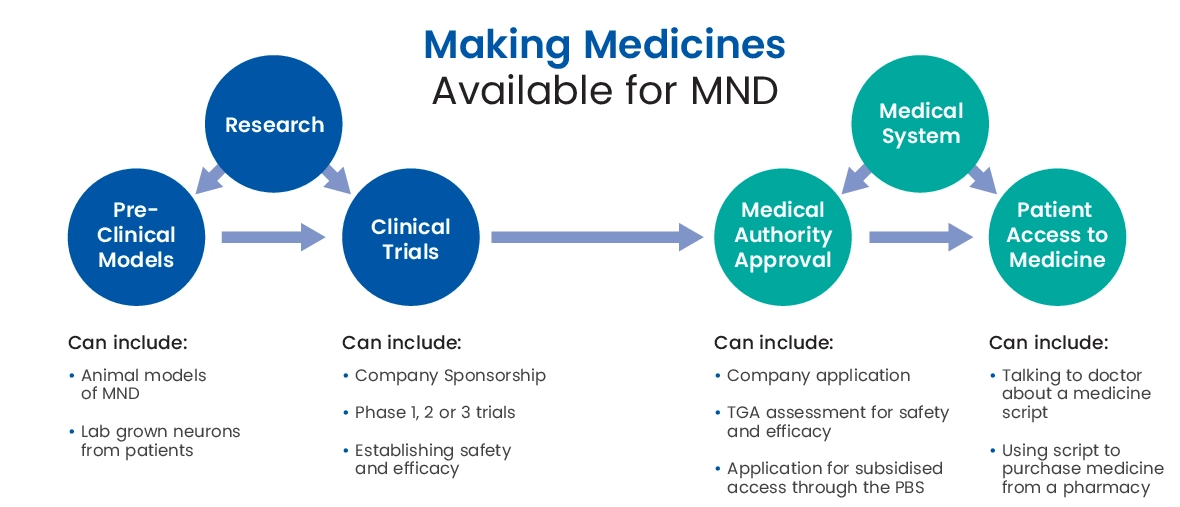
Research is fundamental for developing new medicines and treatments for MND or any other disease or condition. Research is where a medicine for MND begins.
Scientists must rigorously test any potential treatment before its use by patients. First steps in testing often involve seeing if the new treatment works in “pre-clinical models”. Models include lab grown neurons from patients and animal models of MND. If everything looks good after these early steps (also known as pre-clinical testing) the organisation developing the treatment may consider it for clinical trial.
Clinical trials are major research projects.6 Therefore, starting a clinical trial for a potential treatment requires approval. The organisation developing a treatment (usually a pharmaceutical or biotechnology company) is termed the “sponsor” and decides if they think the potential treatment is promising enough to take to trial.
They then apply for approval to the regulatory authorities in the country or countries where they want to run the trial. In Australia, for example, it is the Therapeutic Goods Administration (TGA). In the US it is the Federal Drug Agency (FDA).
Clinical trials consist of phases. Usually, in Phase 1 or Phase 1/2 of a trial, testing determines treatment safety and that it won't cause harm. Scientists may also study what medicine dose might be best (the exact amount taken at one time) as part of the trial.
Phase 1 of a trial is usually very small. The trial will not involve sufficiently higher numbers of participants to provide information on the effectiveness of a treatment. In fact, scientists often run Phase 1 trials on healthy volunteers rather than actual patients. A Phase 2 trial begins after Phase 1 research shows a medicine is safe.
Phase 2 trials mainly aim to finalise the best plan for medicine doses. Trials can also provide some provisional information on the potential effectiveness of a treatment. Scientists often design Phase 2/3 trials to help start understanding treatment effectiveness. Phase 2 trials are larger than Phase 1, especially if they are Phase 2/3, as they gather more data.
It is worth noting: it is not just the decision of the sponsor determining if a treatment progresses to a clinical trial and through all its stages. At each stage data must be presented to the local regulatory authority to show whether the treatment merits progression through the clinical trial pathway.
Phase 3 trials are the final phase of the clinical trial pathway. The trial is the last stage before a sponsor seeks approval to make the treatment available to the public. Scientists specifically design Phase 3 trials to show whether a drug works. The trials need to be much larger than Phase 1 or 2 trials. The reason for the larger size is to establish statistical certainty for definitively saying whether a medicine works or not.
Phase 3 of trials are very expensive (often in the 100s of millions of dollars). In addition to the cost, the trials can take well over 12 months. Trials must be set-up, participants recruited for treatment and analyses conducted. The time and cost are necessary to try and make sure medicines actually work and are safe to use.
From research to pharmacy shelves: making a new treatment available to patients
Once a treatment has been through the clinical trial pipeline and found to be safe and effective, what happens next? How do patients access medicines?
Unfortunately, it is not an automatic progression from trial success to availability to patients. Often, at first glance, the outcomes of clinical trials may appear to be positive. But on closer analysis trial results may indicate that the benefits were not as great as first thought. Conversely, there may have been confounding reasons that resulted in a trial outcome appearing worse than it really was.
To best determine the quality of trial outcomes a local regulatory authority requires the trial sponsor to submit an application for medicine approval. The application allows the authority to objectively and independently review the data.
The authority makes their own decision on the benefit of a particular treatment. Such assessment will involve a number of experts in clinical trials, statistics and the disease area in question.
Assessments are very involved considerations and can often take 6 months or more. As well as considering the effectiveness and safety profile of the treatment, the process considers how medicines are scheduled for prescribing by doctors and whether they are listed on the Pharmaceutical Benefits Scheme (PBS), which helps make medicines available at a lower cost.
Currently, the TGA grants initial approval based purely on whether the evidence shows a treatment is safe and effective.7 The TGA offers very limited opportunity for input into their approval decisions by advocacy organisations such as MND Australia.
The organisation sponsoring development of the medicine completes the application. Some organisations keep applications confidential, making it hard to even know an application is underway. However, in the MND community, which tends to work collaboratively whenever possible, it would be unlikely for an application to proceed without the MND community knowing.
What can help make more medicines available for MND
Clinical trials and regulatory authority approval can take quite a long time. But there are ways to make more MND medicines available sooner.
Ongoing investment in the work of MND scientists in Australia and across the world is critical. Research is best for finding safe and effective medicines that benefit people with MND. Donations, fundraising campaigns and other opportunities to support MND research remain vital for research into medicines.
Beyond research, working with organisations sponsoring medicines can influence the process of TGA approval in Australia. MND Australia and others can, and do, work with sponsors when they are preparing their submissions. MND Australia provides data and brings the experiences of those with lived experience to the table. Sharing data and experience helps to increase the likelihood of approval for a submission.
Working to persuade sponsors to come to Australia, help them understand our system and offer support helps too. Some companies developing new treatments do not have deep resources making targeting multiple countries simultaneously for approval is difficult.
This is the case for Amylyx, the company who developed Relyvrio, which was recently approved for MND treatment in Canada and USA. They need to build up their manufacturing capacity to service the USA and Canada which will establish a steady income stream so they can then look to expand their reach. MND Australia is already scoping how we can best support companies considering applying for medicine approval with the TGA.
In addition to medicine approval, MND Australia and other organisations can help with making medicines more affordable. The application process for subsidised treatment through the PBS does provide an opportunity for organisations to lobby for change.
Lobbying normally takes the form of an organisation completing a written submission about the need for a treatment and its benefits. Organisations submit applications to the TGA review committee. The testimonials of people with or affected by MND can support submissions because they help to share the experiences of daily life from living a terrible disease like MND and why an affordable medicine is so important.
MND Australia are also lobbying for greater involvement of people with MND in TGA decision making more broadly. MND Australia is participating in the review of Australia’s Health Technology Assessment. The review seeks to help reduce the wait times for patients wanting to access new and innovative medicines.
Stay informed
Creating a world without MND, through the search for better medicines, and a cure, is a complicated and difficult challenge. Work is underway though and there are many opportunities to improve access to medicines and life with MND.
It can help to stay informed about what the TGA is considering for MND medicines. Being aware of medicines already available, including Riluzole and medicines for pain relief is important:
- Prescription medicines: applications under evaluation (TGA)
- Riluzole fact sheet
- Breathing and MND: medications and non-invasive ventilation
- Pain management with MND
Doctors, neurologists and other members of the healthcare team for a person living with MND can advise on how to access and use Riluzole and other medicines.